In this issue we take a look at a specific project and examine
its course of development from initial concept to threshold of
commercialization.
- Dave Jaffe tells the story of the Ultrasonic Head
Controlled Wheelchair and Interface.
- Dave follows with a profile of the VA Rehabilitation Unit
in Baltimore. This unit is responsible for evaluating devices developed
within the VA for recommendation within the VA.
- Al Sacks reports on the first meeting of the Tech Transfer
Advisory Board.
- Greg Goodrich and Dave Jaffe report on responses to the first issue of OnCenter.
- Plus - DeVAR in the "garage,"
rehab technology in space, and the
Handbike in the USSR.
A Case Study: The Ultrasonic Head
Controlled Wheelchair and Interface
David L. Jaffe
The design, development, and technology transfer activities associated with
the Ultrasonic Head Controlled Wheelchair (UHCW) has extended over the past ten
years. It has involved my efforts as principal investigator as well as other
researchers, students, test pilots, potential manufacturers, funding agencies,
and personnel from the VA Rehabilitation R&D Evaluation Unit (REU) in
Baltimore. This account briefly documents the history of bringing this design
to commercial reality.
 The student project
The student project
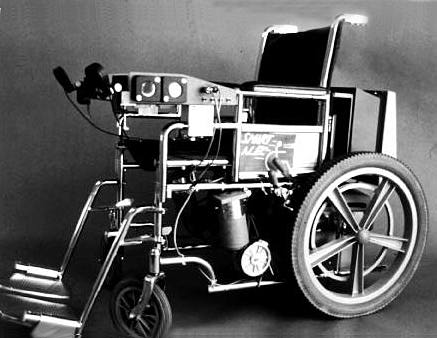
The UHCW project began in October, 1979 at the Design Division at Stanford
University where a group of five graduate mechanical engineering students were
assigned the task of designing an alternative and innovative control and
guidance system for an electric vehicle capable of transporting quadriplegic
individuals. Their nine month effort supervised by me and funded by RR&D
Center resulted in "Smart Alec", a modified Everest and Jennings
electric wheelchair outfitted with shaft encoders, electronics, a
microcomputer, and numerous Polaroid ultrasonic distance ranging sensors. Two
of these sensors monitored the user's head position for navigation while others
detected obstacles in front of, behind, and to the sides of the wheelchair.
After the students graduated and went their separate ways, the project was
moved to the RR&D Center where I continued to refine and publicize the
design. In November of 1980, the project was awarded 4th prize in the Johns
Hopkins Personal Computer Applications Competition in Washington, DC. At the
System Sciences Conference in Honolulu, it was judged the best paper. And in
March of 1981, the wheelchair was demonstrated at the ASME annual conference in
Chicago.
Despite many demonstrations of this new mobility control concept, the
students' solution was far from a practical vehicle. Its deficiencies were
many. The method of loading the computer program from disk storage was both
time consuming and could not be performed by a disabled user. The disk drives
and CRT required a source of AC power during the loading phase, which might not
be available in places where the chair might travel. The software proved
difficult to maintain and modify. Although these problems could not be easily
corrected on the existing prototype chair, the project did show the feasibility
of computer controlled mobility directed by head position. It also showed that
the ultrasonic sensor system could detect obstacles and take appropriate
action. The practical execution of these concepts would have to be accomplished
in a later design.
Second generation design
Since the ultrasonic head control technique appeared to have sufficient merit
for further development, I decided to pursue a generalized wheelchair
interface. A proposal was submitted to and funded by the Technology and
Research Foundation of the Paralyzed Veterans of America for this work. In May,
1982 the Ultrasonic Head Control Unit project was begun at the RR&D Center,
its goal being the development of a second generation wheelchair control
system.
With that funding, advances in computer hardware, and new developments in
high level programming languages, a new Ultrasonic Head Controlled Wheelchair
was developed by the first half 1983. The computer's instructions were then
permanently stored on a memory chip and the entire computer was powered by the
wheelchair's batteries. A more accurate and faster technique of acquiring head
position information improved the steering and control characteristics. In May,
1983 the first disabled user test drove the new design and in June it was
demonstrated at the RESNA conference in San Diego. A dozen quadriplegic
patients at the Palo Alto VA Spinal Cord Injury Service subsequently tested the
prototype.
In response to many technical inquires about the wheelchair, I compiled a
sixty-five page Technical Manual. It contains complete descriptions of the
workings of the UHCW, including schematics, wiring diagrams, computer program
source code, and parts list. With this document a knowledgeable engineer in an
adequately equipped laboratory could duplicate the head controlled wheelchair.
In the past five years over one hundred investigators, researchers, and
interested manufacturers world-wide have received copies of the manual.
In 1985, as work was progressing on a voice controlled mobile robot,
modifications to the wheelchair-mounted head control unit were made to enable
its use in specifying movement trajectories. This capability would allow the
severely disabled user to control complex robot movements using only head
motions.
Despite continuing interest in the wheelchair and ultrasonic distance
ranging technology, no manufacturer had stepped forward to pursue commercial
development of the design. In mid-1985, the Rehabilitation R&D Evaluation
Unit (REU) was formed within the VA system. (For a description of REU, see the
related article in this newsletter.) A Request for Evaluation for the UHCW from
RR&D was one of the first to be received and approved by this new agency.
The evaluation contract
The proposal called for the development and delivery of four pre-production
UHCW devices. These units were to be clinically tested at VA Medical Centers
around the country for certification. It was not until 1987 that the funds were
received and contracted to Eureka Laboratories of Sacramento, CA as the result
of a competitive bidding process. The company was initially made aware of the
RR&D Center's work during a Manufacturer's Conference organized jointly by
the VA and the Department of Commerce. In one-year's time Eureka completely
redesigned the UHCW, taking advantage of new microcontroller technology and
incorporating safety and design features necessary of a production device. A
packaging upgrade to improve the aesthetics was also accomplished. Their
initial device underwent a successful local acceptance test in June, 1989 and
was delivered to REU shortly thereafter.
Under the REU program, clinical evaluation is to be accomplished at several
VA facilities. A protocol has been developed by REU encompassing testing
methods, questionnaires, subject selection, and data collection methods. The
process is estimated to take about one year and if successful, will result in
an approval for VA physicians to prescribe the UHCW for quadriplegic veterans.
By virtue of their early involvement in this project, Eureka will be in a good
position to fill any orders for UHCW's submitted by the VA or other third-party
payers.
While the events described above may not be typical or even necessary for
other projects, they do show what it takes bring a good project idea to the
point of commercialization: a concerted, long-term technical effort, several
infusions of funding, and plenty of patience on the part of RR&D Center
investigators. This case also illustrates the advantage to all parties when
manufacturers become aware of projects in their early stages. The R&D team,
the manufacturers and the end user all benefit from this early involvement.
Advisory Board provides technology transfer
expertise
Alvin H. Sacks and Gayle Curtis
The recently formed Technology Transfer Advisory Board held its first
meeting at the VA Medical Center in Palo Alto on October 25, 1989. The Board
consists of twelve non-government specialists in the fields of technology
licensing, patent and Federal law, marketing, third party payers, product
design, venture capital, rehabilitation medicine, rehabilitation service
delivery, manufacturing, and business. Three of these Board members are
themselves users of rehabilitation devices.
The purpose of this half-day joint meeting of the Advisory Board and our
internal Technology Transfer group was to develop an overall program to
maximize technology transfer of products and processes developed within the
RR&D Center here.
Two issues emerged as central to the tech transfer process. The first is:
What is success? What are the measures of success and how do they differ for
research professionals, institutions and end users? The second issue is
related: How to pick projects, both to develop and to support for tech
transfer? What informs this selection process? These issues sparked a great
deal of lively participation, since they have no easy answers, and nearly
everyone has an opinion. From this discussion it was clear that the board could
offer expertise and support in many areas, particularly in those of planning,
patents, industrial contacts and agreements.
The group decided to meet quarterly and to hear about individual products or
projects from the Center presented by the product "champion", usually
the Principal Investigator or principal designer on the project. This will
enable the Board to critique the project and to assist in developing a
technology transfer approach specific to that product. Board members also
expressed their interest n consulting individually with project champions to
help implement a particular technology transfer approach for that project.
The Advisory Board held its second meeting on January 31, 1990. The board
heard a brief status report on four of our projects which are nearing
commercialization: the Ultrasonic Head Controlled Wheelchair/ the Handbike, the
Computerized Visual Communication System and the Traction Backboard. Discussion
then opened to the general concerns of the group around technology transfer and
the key questions it raises. The third Advisory Board meeting is planned for
early June.
The Rehabilitation Evaluation Unit:
facilitating technology transfer for VA RR&D Centers
David L. Jaffe
One of the most challenging aspects of the rehabilitation research and
development process is the transfer of laboratory prototypes from the Palo Alto
VA's Rehabilitation Research and Development Center (RR&D) to private
companies for manufacture. Without a purposeful program of technology transfer,
devices developed by RR&D would remain mere research curiosities and would
not benefit disabled veterans.
To assist in the technology transfer of promising devices and techniques
developed at RR&D, the VA has established the Rehabilitation R&D
Evaluation Unit (REU) in Baltimore, MD. The main function of the REU is to
assist RR&D Centers in their prime responsibility - making effective
devices and techniques available to veterans. The REU evaluates candidate
devices for use within the VA system. Devices approved by the REU may be
recommended, prescribed and purchased for use by disabled veterans.
Request for evaluation
Central to process of technology transfer is the interaction and ongoing
communication between RR&D investigators/ REU personnel/ potential
manufacturers/ and clinical evaluators.
Through reports and personal conversations REU knows of progress in
RR&D/s projects as they approach the research prototype phase. When a
project reaches the stage where a working prototype has been constructed, the
investigator, in consultation with REU, can submit a "Request for
Evaluation" proposal to REU. This document describes the current state of
the research/ gives specifications for commercial prototypes/ and includes a
budget for constructing a small number of the devices. These devices will be
used in the subsequent evaluation process.
The REU reviews the Request for Evaluation, and if approved, supplies funds
to the Palo Alto VA Supply Service. This department then initiates an open
competitive bidding process by publishing a solicitation request. The responses
of interested companies are judged and the lowest competent bidder is awarded a
one year contract to construct several pre-production devices for evaluation.
Since this process is open to small and minority businesses as well as
companies not necessarily involved with devices for the disabled, this activity
attracts new manufacturers to the rehabilitation field.
Contract
During the contract phase, the manufacturer and the RR&D investigator work
closely together to transfer expertise acquired during the research and
development phase. Frequent conversations and visits are typically needed
during the year to monitor progress towards the development and construction of
the prototypes.
During the contract year, REU investigators, in collaboration with the
RR&D investigator, formulate a clinical evaluation protocol. This includes
the selection of clinical evaluators at VA Medical Centers or at facilities
outside the VA system. It also includes the production of a study plan with
instructions for the clinicians, questionnaires, human subject selection
criteria and approval forms, evaluation methods and data collection forms.
At the end of the contract, and prior to acceptance and shipment to REU, the
resultant devices are inspected to insure they meet the specifications outlined
in the solicitation. When the contractor's devices arrive at REU, they are
tested once again for function, reliability, safety, and compliance with design
specifications. Additional modifications may be required to achieve these
goals.
Evaluation
The formal evaluation at the selected sites then begins. This activity benefits
both the VA and the manufacturer who anticipates full-scale production. For the
VA, it is a chance to clinically test new devices in a controlled fashion,
making sure they meet a real need. For the manufacturer, it is an opportunity
to have their device included on an accepted list from which VA physicians
prescribe. The VA Prosthetics and Sensory Aids Service also purchases equipment
for disabled veterans from this list. The evaluation also results in training,
fitting, and clinical information for practioners, non-veteran consumers and
third party payers.
Although technology transfer could occur without REU's participation, this
process provides a mechanism for involving commercial companies and encouraging
them to manufacture devices for the disabled community. The funds that REU
provides might not otherwise be available to a small company wishing to enter
the rehabilitation field. This evaluation process therefore stimulates
technology transfer by supporting the construction of pre-production units
based on RR&D prototypes. Devices that pass the subsequent evaluation are
certified for prescription for disabled veterans. The final result is that a
significant number of disabled individuals, both veterans and non-veterans, can
be provided with new and improved devices.
Tech Transfer information briefs
Gayle Curtis
DeVAR in the High Tech Garage
The RR&D Center is working with the Technology Center of Silicon Valley to
develop a robot exhibit for their new "High-Tech Garage." This
facility will introduce visitors to evolving technology through interactive
exhibits and educational programs designed to make the technology less
mysterious and more accessible.
We are helping to develop an exhibit which will show human service
applications of robots. This exhibit will be patterned after our DeVAR Robotic
Aid and will feature a PUMA robot in a vocational and daily living setting. We
are providing expertise and a human-values perspective to this component of a
large installation featuring robotics. Other components will highlight the
speed and flexibility of industrial robots.
Space exploration, microelectronics, superconductivity, biotechnology,
CAD/CAM, bicycles, materials technology, as well as robotics, will all have
exhibits in this opening installation in the "High-Tech Garage."
Rehab technology in space
Doug Schwandt, a biomedical engineer at the Rehabilitation R&D Center, has
been working with NASA-Ames Research Center to develop exercise equipment for
astronauts to minimize deconditioning due to exposure to microgravity. Drawing
upon his experience with mobility, exercise and recreation equipment developed
at the Rehabilitation R&D Center, Doug has developed several exercise
equipment concepts which may in turn be useful for rehabilitation here on
Earth.
Handbike in the USSR
Design USA, a cultural exchange exhibit sponsored by the US Information Agency,
is on a nine-city tour of the Soviet Union. By invitation, the Handbike
represents products developed here at the Rehabilitation R&D Center in a
"Design for Special Needs" section of the exhibit. Well over 500,000
Soviet visitors have already viewed the exhibit since it opened in Moscow and
Leningrad. Doug Schwandt, principal designer of the Handbike, will participate
as a "Designer in Residence" and help organize a Special Needs Design
Seminar.
C-VIC licensing agreement signed
Richard Steele, an investigator at RR&D Center, reports that he and the
other inventors of the Computer-aided Visual Communication system (C-VIC) have
just signed a licensing agreement for its commercialization and distribution.
This software application, which runs on an Apple Macintosh (TM) computer,
enables communication with interactive visual symbols for those who have lost
the ability to use language. More details in the next issue of OnCenter.
 DeVAR in evaluation
DeVAR in evaluation
The Desktop Vocational Assistant Robot (DeVAR) is currently undergoing field
evaluation at a site in San Francisco. Bob Yee, a senior programmer/analyst
with Pacific Gas and Electric (PG&E), is a disabled veteran who uses the
robot for many tasks an attendant would normally perform, such as tearing off
print-outs, feeding him lunch, and answering the phone. This field trial,
underway since September 1989, will provide valuable information about the
effectiveness of the robot as a vocational assistant.
Who reads OnCenter?
Greg Goodrich and David L. Jaffe
The OnCenter newsletter is designed to inform our readers of new research
developments and technology transfer activities at the RR&D Center. It is
distributed to researchers, manufacturers and professionals in the
rehabilitation community. Which the premier issue we mailed a Subscription
Qualification Form which included a questionnaire to learn more about our
readers, their interests and areas of specialization.
The questionnaire requested information on the type of business or service
provided, age and disability group targeted, type of rehabilitation products of
interest to our readers, and other questions. As of this writing (January 1990)
over 900 responses have been received from a mailing of over 2100 with more
arriving daily. The first 600 responses received were analyzed in detail.
The returned questionnaires indicated that OnCenter readers are a diverse
group, representing the breadth of companies, agencies, and professions that
make up the rehabilitation community. Readers responded from 12 countries,
forty-two states, and the District of Columbia. Eighteen respondents listed
their affiliation as television, radio, or print journalism, indicating that
the media actively seeks information from the rehabilitation community for
dissemination to the general public.
Most responding readers (89%) were affiliated with either manufacturing,
marketing, distribution, research and development, technology transfer,
education and training, client services, or rehabilitation. For analysis we
grouped the responses from these eight areas into three more general categories
- 1) Development - research & development, technology transfer, 2) Delivery
- manufacturing, marketing, distribution, and 3) Dissemination - client
services, rehabilitation, education & training.
Development Delivery Dissemination
Age Level
Infant 18 14 19
Child 28 28 27
Adult 32 33 33
Senior 22 24 21
Disability
Hearing 13 9 15
Sight 15 13 15
Paralysis 21 23 19
Aging 13 15 13
Brain Injury 18 18 19
CP/MD/MS 20 21 20
Table 1. Responses (in %) by response category: development, delivery, or
dissemination.
In examining the responses, we find that 27% fall in Delivery, 22% in
Development, and 52% in Dissemination. Table 1 shows the percentages of
responses for the categories defined above for the various age levels and
disability groups. Figure 1 shows the distribution among the six product
classes.
This survey profiles the interests of our readers - it shows a strong
interest in mobility and communication, and indicates that the interests of
those dealing with users of rehabilitation technology are different from those
who develop and deliver that technology. We will conduct future surveys to
characterize these differences in more detail. Through this newsletter and
questionnaire, we aim to identify unmet needs for rehabilitation technology and
potential technology transfer partners.
Product Phase Delivery Development Dissemination
Communication 22 17 22
Sensory Aids 26 33 20
Recreation 14 13 16
Mobility 15 14 14
Manipulation 12 10 13
Info. Access 13 15 17
Figure 1. Responses (in %) by product class
For more information on any of these articles, contact the author at
650/493-5000 ext. 6-4475.